")

Can AI Eliminate “Dead Time” in Drug Development?
FDA’s Emerging Vision for Real-Time Clinical Trials
Clinical development timelines continue to stretch, driven not only by trial complexity, but also by the growing administrative and reporting burden between studies. To address this challenge, FDA recently announced a two-part initiative to begin advancing real-time clinical trials (RTCT) in early phase drug development. Although still in its infancy, this initiative has the potential to leverage advances in artificial intelligence (AI) to transform how clinical trials are conducted, ultimately accelerating the delivery of safe, life-saving medications to patients.
This post explores the underlying problem, FDA’s proposed solution, and the key considerations and issues that may shape the successful implementation of RTCTs.
Current Problem: The Growing Dead Time Between Clinical Trials
One of the most underappreciated and addressable drivers of prolonged development timelines is the growing gap between clinical trial phases. FDA has termed this “dead time.” Over the last 10-15 years, the amount of time spent between clinical trials, including administrative closeout and key decision points, has significantly increased. Several reports found that study closeout time has increased three- to fivefold over the last 15 years.¹˒²
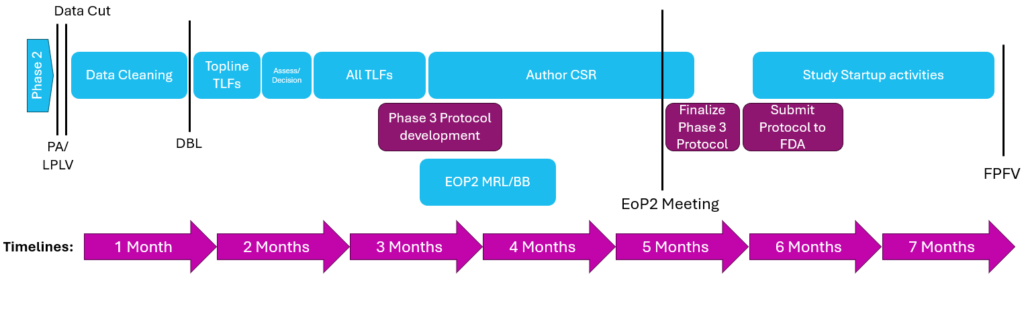
The typical steps between trials include data cleaning, analysis, and generation of topline tables, listings, and figures (TLFs), followed by preparation of reports to support development decisions (Figure 1). This process is time-consuming and often inefficient, resulting in fragmented data flow, redundancy, and increased potential for errors, all of which contribute to prolonged timelines.
Goal of Real Time Clinical Trials (RTCT)
Real-time clinical trials (RTCT) aim to enable continuous data sharing and evaluation between sponsors and FDA during an ongoing study rather than after study completion, with the goal of reducing “dead time” between clinical trial phases.
To enable RTCT, FDA is proposing the use of AI to support clinical trial monitoring activities. Under this model, study sites would enter data into a shared environment accessible to sponsors and FDA. AI tools could analyze the data and flag potential safety signals or efficacy trends based on predefined criteria outlined in the protocol and statistical analysis plans (SAP). Sponsors and FDA would use this information to make regulatory decisions. This approach enables earlier and more continuous assessment, potentially months to years ahead of traditional reporting timelines.
FDA’s Current and Future RTCT Plans
To test the feasibility of RTCT, FDA has already announced the initiation of early proof-of-concept studies while laying the groundwork for broader implementation. To maintain trust and ensure patient safety, these programs are expected to run RTCT in parallel with the traditional reporting system, ensuring no safety signals are missed and allowing for direct comparison and validation of this new approach.
Current RTCT Proof of Concepts Studies
The two proof of concept studies include a:
- Phase 2 open-label study (TrAVeRse, NCT05951959) evaluating treatment in patients with treatment-naïve mantle cell lymphoma, and a
- Phase 1b trial (STREAM-SCLC) evaluating treatment in patients with limited-stage small cell lung carcinoma.
This selection likely reflects a strategic choice by FDA, as early phase, open-label oncology studies, typically generate frequent safety signals while minimizing the risk of unintentional unblinding.
Future RTCT Pilot Program
On April 28th, 2026, FDA announced that an RTCT pilot program will be launched in summer 2026. In preparation, FDA has released a request for information in the Federal Register seeking feedback on key aspects of the programs. FDA is asking for any input to these questions by 29th May 2026 end of day.
Key Considerations for Successful RTCT Implementation
As discussed above, RTCT monitoring offers an innovative way to utilize the advancements in AI to decrease clinical trial timelines. However, to take full advantage of the promises associated with RTCT, several key considerations must be addressed by FDA and industry stakeholders.
Identifying the Most Appropriate Initial Use Cases
One key consideration is to identify and define the most appropriate study types for RTCT monitoring. Because the RTCT process involves sponsors and FDA gaining access to real-time, patient-level data, there is an increased risk of unintentional unblinding, which would affect trial and data integrity. To mitigate this risk, implementation of RTCT may be better suited to early-phase open-label studies. Focusing on these studies could enable the benefits of RTCT while accelerating early drug development and avoiding the complexities associated with blinded trials, where safety and efficacy findings can inform pivotal marketing decisions. FDA’s two proof of concept studies appear to support this approach, as both are Phase 1 or Phase 2 open label studies. As experience with RTCT grows, it will be interesting to see if this model can work for double-blind approaches in the future.
Operational Scalability
Another consideration is scope, as it is unrealistic to expect RTCT to apply to all clinical trials. As of May 2026, more than 86,000 clinical trials are listed as active on clinicaltrials.gov, likely an underestimate given that Phase 1 studies are not required to be registered. Under the current models, sponsors assess and report safety and efficacy findings. Transitioning to AI-assisted systems could increase reporting volume, including false positives, potentially straining FDA resources. Therefore, careful consideration must be given to defining the scope of RTCT implementation.
Building Confidence in AI-Assisted Monitoring
Establishing trust in AI systems among regulators, sponsors, and the public is also critical. The first step in ensuring trust is determining how the AI will be trained. This process will require careful consideration to ensure no bias that would impact how the AI analyzes safety and efficacy data. Additionally, validation, ongoing performance monitoring, and comparisons with traditional methods will be required to ensure AI systems meet the same level of rigor as existing processes. These requirements would likely introduce significant costs and resource demands for the FDA, which must be considered in long-term planning.
Conclusions and Future Process
RTCT represents a promising evolution in clinical trial oversight enabled by AI, with the potential to support more continuous insight generation and faster decision-making. Its success will depend on balancing innovation with regulatory rigor. Key considerations, including defining appropriate scope, managing increased regulatory burden, preventing unintentional unblinding, and establishing trust in AI-driven systems, should be addressed through ongoing evaluation.
RTCT offers a meaningful opportunity to reduce inefficiencies in clinical development and reshape how sponsors and regulators interact. A thoughtful, evidence-based approach will be essential to realizing these benefits while maintaining the safety and integrity of clinical trials
References
- Culbertson J. Clinical trial duration trends & the study closeout gap. Clinical Leader. Published June 14, 2022. Clinical Leader article
- Tufts Center for the Study of Drug Development. Faster new drug approval times are more than offset by longer clinical times in U.S., according to Tufts Center for the Study of Drug Development [press release]. GlobeNewswire. Published July 16, 2020. GlobeNewswire press release




